
 This article was published in Australian Doctor in the “Grand Rounds” segment. It was titled “Context is crucial” in the printed version, and “Over-anticoagulation: when adherence to guidelines is not always the wisest course” in the online version.
This article was published in Australian Doctor in the “Grand Rounds” segment. It was titled “Context is crucial” in the printed version, and “Over-anticoagulation: when adherence to guidelines is not always the wisest course” in the online version.
Authors: Patrick Khoury and Michael Tam
This article is also available on the Australian Doctor website (registration required).
Case
Mrs B was a pleasant 65 year old lady, living with a diagnosis of scleroderma, and a long term patient of the General Practice Unit. She presented with a centimetre diameter ulcer on the left calf. There was no discharge or erythema – it was not infected. There were skin changes consistent with scleroderma (dry thickened skin, loss of hair, hypo- and hyper-pigmented areas), and marked varicose veins.
The immediate working diagnosis was a venous ulcer, but a deep venous thrombosis was suspected. Mrs B had a tender calf and had recently been admitted for a few days in hospital for an unrelated complaint. The DVT was confirmed on venous duplex ultrasonography – there was thrombosis of the left posterior tibial vein, along with extensive thrombosis of the long saphenous vein.
Initiating anticoagulation
After a discussion with the patient and her rheumatologist, it was agreed that anticoagulation should be initiated immediately – warfarin, with low-molecular weight heparin (enoxaparin, or Clexane) cover. I (PK) hadn’t commenced warfarin in the general practice setting before, so I made use of eTG Complete (Therapeutic Guidelines Ltd) – a resource to which I was very familiar.
I followed the “Age-adjusted warfarin initiation protocol (Appendix 3.1)” in the cardiovascular guideline [1]. Day 1 (Thursday) – warfarin 9 mg dose. Day 2 (Friday), Mrs B’s INR was 1.3 – another 9 mg dose.
That afternoon, I realised that there was a looming problem. The protocol required daily INR results and we weren’t open on the weekend! I spoke to my supervisor, who perceived the dosing was too aggressive. He suggested that Mrs B take 5 mg daily on the weekend (days 3 & 4), and to measure the INR early Monday morning (day 5). His gut feeling turned out to be right – the INR was 5.4.
Management of over-anticoagulation
Luckily, there was no evidence of bleeding and Mrs B was otherwise feeling well (if bemused)! I turned to eTG Complete again, and found the section on “Management of bleeding and/or over-anticoagulation”; it recommends for INR 5-9 to give vitamin K – either orally or IV. [2]
Feeling anxious from my recent experience, I sought help. Both my supervisor and another senior GP instinctively felt that vitamin K in this situation was the wrong approach. They recommended that we should withhold a dose of warfarin and to repeat the INR the next morning. With some trepidation, I followed their advice and gave extensive safety-netting advice with regards to bleeding.
Happily, the INR the next day was 2.5. Crisis averted! Mrs B’s ongoing stable dose of warfarin has been 2.5 mg daily.
Discussion and reflection
eTG Complete is an extremely useful set of Australian treatment recommendations and guidelines, and is a resource that I use frequently. Thus, I was initially flummoxed by what seemed to have been inappropriate advice, twice, in the guidelines.
On reflection, the problem related to my assumptions about guidelines. eTG Complete is written in a style that is clear and relatively minimalistic, which is perhaps why it is much loved by junior doctors. However, beneath the simplicity, no guideline is free from contextual constraints. For instance, although the over-anticoagulation guideline does not state it explicitly, it assumes that bleeding risk is high (reasonable for hospitalised patients) – thus the recommendation for vitamin K. The source guideline that eTG Complete references provides more detail and nuance – where bleeding risk is not high (typical in community patients) vitamin K is usually unnecessary for INR 4.5 to 10. [3]
Similarly, the warfarin initiation protocol assumes that INR can be easily measured at a specific time each day, and aims to rapidly achieve INR target levels. Again, this is reasonable for patients who may be otherwise waiting to be discharged from hospital, but is less practical in general practice settings.
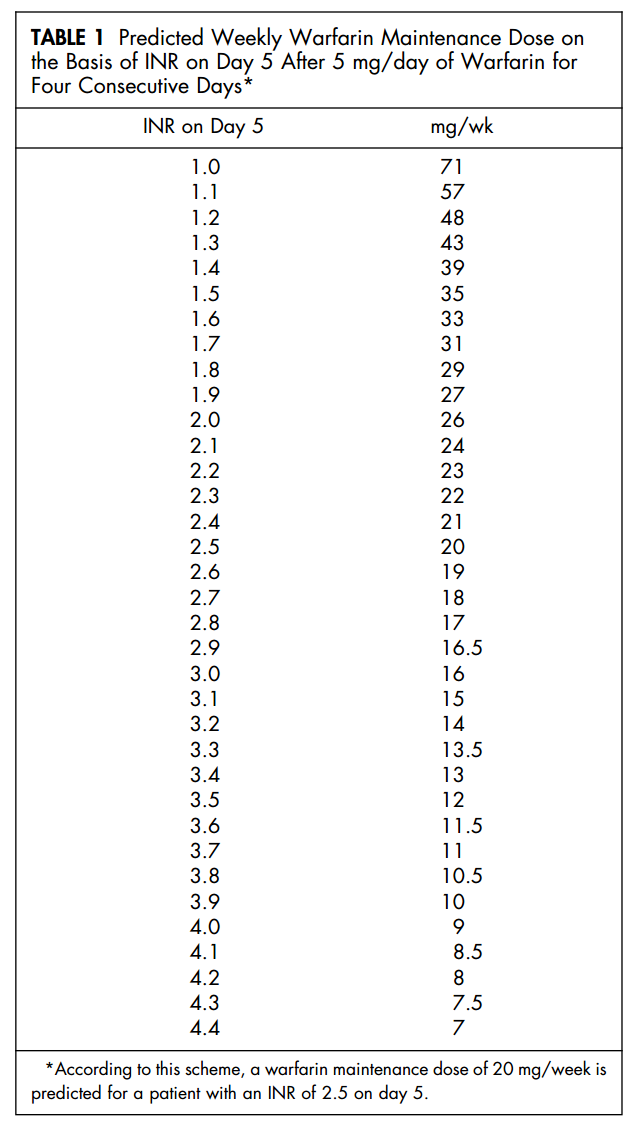
Rather, rapidly reaching the target INR is a lesser priority, while avoiding highly elevated INR results an important one. Pragmatically, it may be better in general practice to preference a warfarin initiation strategy that maximises safety, and requires fewer INR measures. For instance, one very simple protocol involves four consecutive daily doses of 5 mg – the INR level on day 5 reliably predicts the ongoing dose (see Table 1 from Pengo et al, 2001). [4]
This clinical scenario reinforced for me the importance of contextually applying guidelines and evidence to individual patient care, and to not just follow a protocol uncritically.
References
- Age-adjusted warfarin initiation protocol (Appendix 3.1) [revised February 2012]. eTG Complete (etg43 November 2014). http://etg.tg.com.au/ip/desktop/index.htm
- Management of bleeding and/or over-anticoagulation [revised February 2012]. eTG Complete (etg43 November 2014).
- Tran HA, Chunilal SD, Harper PL, Tran H, Wood EM, Gallus AS. An update of consensus guidelines for warfarin reversal. Medical Journal of Australia 2013; 198(4): 198-199.
- Pengo V, Biasiolo A, Pegoraro C. A simple scheme to initiate oral anticoagulant treatment in outpatients with nonrheumatic atrial fibrillation. The American Journal of Cardiology 2001; 88(10): 1214-1216. http://dx.doi.org/10.1016/S0002-9149(01)02069-0